
Post 15: Primary Palliative Care
Framing why communicaqtion skills are important for EVERYONE

As many of you may know, besides being an oncologist, I am a Hospice and Palliative Medicine (HPM) clinician. Most of my work in the HPM field is in communication skills research and patient centered care. “Meaningful Conversations” and the work on this substack is an effort to improve patient centered care.
Here are some observations and learnings from my twenty year career learning and teaching communication skills.
The principles of meaningful conversations has been part of medical training since the beginning of time; as they are fundamental to “caring.”
Over the past few decades, there has been increasing fragmentation in care.
Evidence suggests that early integration of palliative care into routine oncological care improve “care of the patient.”
There are not enough palliative care doctors in the country to meet the needs of our patients, our family and our community.
To meet the needs of our patients, our familiy, and our community, we need to divide the workload across primary and subspecialty care.
Primary Palliative Care (PPC) is an important solution to meeting the need of our patients.
What is Primary Palliative Care?
Palliative care refers to care focused on “alleviating” or “palliating” patient’s symptoms. Symptoms can be divided into various different domains including: physical, emotional, and spiritual well being. Delivering palliative care involves assessing for symptoms within these domains and helping patients with decision making that is centered around their goals, values and preferences. Meaningful Conversations, or what we are doing in these posts, is focused on doing just that.
Primary Palliative Care refers to the care where the symptoms are assessed and addressed by the primary team (primary care doctors, cardiologist, oncologist, pulmonologist etc). Subspecialty Palliative Care refers to the care where the symptoms are assessed and addressed by fellowship trained palliative care providers.
What is addressed by the Primary Palliative Care teams?
Along with my colleagues, we published model for integration of palliative care into routine kidney cancer care. The figure below is an example of how to visualize and implement primary palliative care.
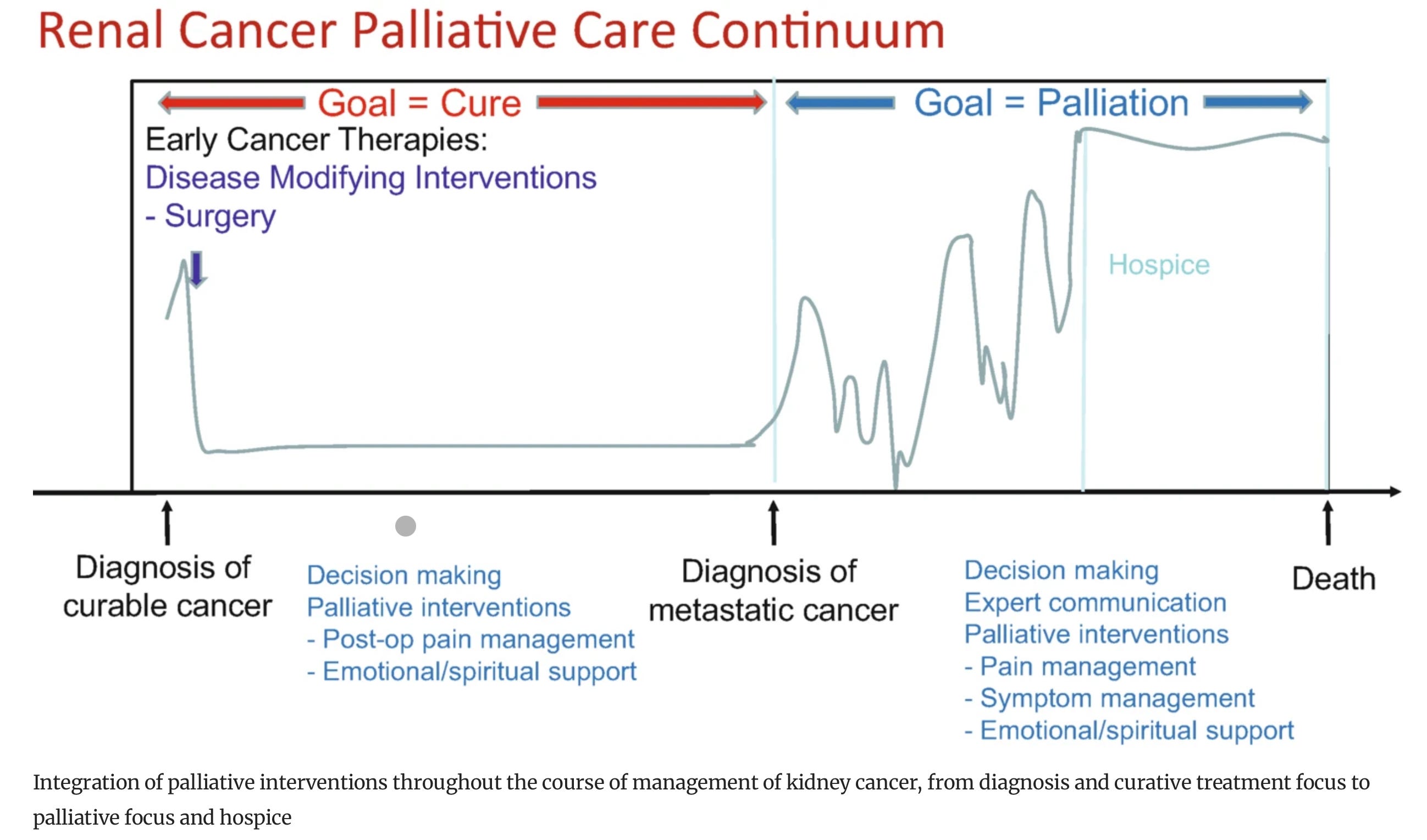
Source : Wilton et al., 2023
Most patients will meet with urologist for localized kidney cancer and discuss that it is “curative disease” and treatment choices include surgical resection, observation or other local therapies as standard of care. So in this case, the shared decision-making, palliation of potential symptoms (pain, bleeding) are managed y the primary urologist or urologist oncologist. Post-operative pain and emotional and spiritual concerns may also be addressed by the primary team. The team members can include: Urology/urologist oncologist, nursing staff, social worker or other members of the clinical team.
A few patients will present with metastatic disease or will progress to have cancer recur after curative intent therapies. Thus the focus is on “palliation” of cancer and its treatment. Here, some of the same functions need to be accomplished. Decision-making about how to address the cancer (using expert communication skills and SDM philosophy), along with assessment and treatment of symptoms from cancer are some of the palliative interventions that can be (should be) performed by the primary oncology team that can including urology oncology, medical oncology, radiation oncology and if needed palliative care team.
In a system where the initial symptoms and discussions about SDM and goal oriented care can be accomplished by the primary team(s), palliative care team can serve as the subspecialist and help the primary care when needed.
What skills do the Primary Palliative Care teams need?
To provide the primary palliative care to their patients, first and foremost the team needs communication skills to elicit patient goals, values and preferences. They need the skills to ensure the patient and family “hear” all of the options including risks and benefits of each of the options. They can then help select the optimal choice based on what is iportant for the pateint.
Primary palliative care team also needs to have the skills to evaluate each potential symptom (physical, emotional and spiritual) and provide support and/or address them appropriately.
The primary palliative care team also needs to recognize when they are not able to address any of the above symptoms or patient needs and seek help from the subspecialty palliative care teams.
Take aways:
Each of us needs to have adequate skills in communication skills to help patients with goal oriented SDM.
Each of us needs to be mindful of when we need help and seek the help to ensure patient’s needs are met.
The analogy that we use often is that , say a patient has Hemoglobin of 5, would you just call GI and not transfuse until then or say someone has A fib not correct that while awaiting a cardiologist consult.
Communications skills with others are no different infact they are the catalyst for meaningful conversation...